On This Page
Breast reconstruction can be a life-changing procedure for patients looking to restore breast shape and symmetry following mastectomy. During a consultation with Dr. Aya-ay, patients can determine whether breast reconstruction is the procedure best suited to their needs.
What is Breast Reconstruction?
Breast reconstruction is performed following a mastectomy, or removal of the breast. The most common indication for breast reconstruction is to reconstruct the breast after the diagnosis of breast cancer. Some women will also undergo prophylactic mastectomy when they are deemed high risk for breast cancer and/or have the genetic susceptibility to breast cancer.
Plastic Surgery is a key component in the multidisciplinary approach to the care of breast reconstruction patients. A patient who is considering a mastectomy for the treatment of their cancer or for prophylactic purposes should have a consultation with a plastic surgeon to discuss options for reconstruction.

Melanie L. Aya-ay, M.D.
BOARD-CERTIFIED PLASTIC SURGEON
Dr. Melanie Aya-ay is a board-certified plastic surgeon in Tampa Bay with over 15 years of plastic surgery experience specializing in cosmetic surgery, reconstructive breast surgery and minimally invasive techniques for facial and body rejuvenation. She is known for her skill and excellence in revision surgery, specifically for difficult breast surgery revisions. Dr. Aya-ay is an Allergan Medical Institute (AMI) National Trainer for Facial Aesthetics and AMI National Speaker for Plastic and Regenerative Medicine. She is honored to be the first female surgeon to hold this dual faculty position with Allergan.
Dr. Aya-ay is the CEO and owner of Melanie L. Aya-ay, MD Plastic Surgery as well as Vivia MedSpa, an elite luxury medical spa in North Tampa. Her practice and her team have been built on the values of honesty, integrity, education, safety, and providing comprehensive aesthetic care with natural results. Your consultation with Dr. Aya-ay will be an educational experience so that you can be assured that you are making the choices that are best for you. Our staff will provide all the assistance needed to help you navigate through the process for a successful Plastic Surgery experience.

Breast Reconstruction Procedure
In general, breast reconstruction consists of a series of surgeries that occur in a staged fashion. The first surgery may be performed at the time of the mastectomy, which is known as immediate breast reconstruction. Delayed immediate reconstruction is sometimes recommended for a patient. In this case, the first stage of reconstruction is performed 2-3 weeks after the mastectomy. In more advanced stages of disease, cases that require radiation therapy, or if it is the patient’s preference, breast reconstruction can be completed in a delayed fashion months or even years after the mastectomy.
The breasts can be reconstructed using tissue expanders and implants or with the use of the patient’s own tissue, known as autologous reconstruction. In autologous reconstruction, the most common flaps used are the latissimus dorsi myocutaneous (LDMF) flap, the transverse rectus abdominis myocutaneous (TRAM) flap, or the deep inferior epigastric perforator (DIEP) flap.
In some patients, the nipple and areola can be saved with what is known as a nipple-sparing mastectomy. To be a candidate for a nipple-sparing mastectomy, the patient must meet criteria from both an oncologic (cancer) perspective and from an aesthetic standpoint. Many patients are not a candidate for a nipple-sparing mastectomy and therefore undergo a skin-sparing mastectomy. For these patients, a nipple and areola are reconstructed at a later staged procedure.
For women who chose to have a unilateral mastectomy, a symmetry procedure may be needed in the native opposite breast to provide the best aesthetic result. A symmetry procedure may consist of an augmentation, mastopexy, or breast reduction. Women who choose breast conservation therapy with a lumpectomy may have significant asymmetry that could benefit from a symmetry procedure. In most cases, symmetry procedures are standard in the care of the breast cancer patient and usually are covered by their health insurance plan.
During your consultation, Dr. Aya-ay will discuss these options with you, and together you will decide which form of breast reconstruction is best for you.

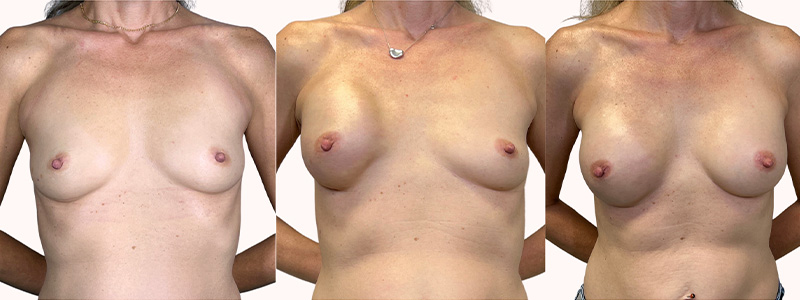
Beautiful, Natural, Results.
BEFORE AND AFTER PHOTOS
Breast Reconstruction Recovery and Aftercare
The patient’s time of discharge depends on the type of surgery they receive. Patients who have implant surgery are typically discharged within two days. Those who receive autologous reconstruction, or reconstruction using the patient’s own tissue, will typically be able to return home within 5 days after the surgery is completed. Patients may experience swelling and bruising for up to 8 weeks following the procedure.
Patients can expect to be discharged with a dressing in place, as well as either a wrap bandage or a surgical bra to provide support and help minimize swelling at the site of the procedure. Depending on the type of surgery that is performed, patients can expect to return home with a drain in place, which serves to prevent excess fluid during the healing process. The removal date for the drain or drains will be determined in consultation with Dr. Aya-ay.
During the period of recovery, the patient will have activity limitations in order to decrease the risk of postoperative complications. Postoperative medications may include an antibiotic, pain medication, and an anti-nausea medication to be used as needed. Dr. Aya-ay and her staff will review the postoperative instructions with you at your consultation and again at your preoperative visit to ensure that you are comfortable with your postoperative care.
Schedule a Consultation
To learn more about breast reconstruction or other potential options, schedule a consultation appointment with Dr. Aya-ay. A consultation is a chance to collaborate to decide what procedure or treatment would be best suited for you and your needs. To schedule your consultation appointment, contact our Tampa office.
